THE ORIGINAL ARTICLE CAN BE FOUND HERE
What to expect when you’re expecting an extra X or Y chromosome
Prenatal genetic tests can detect sex chromosome aberrations, but what happens after—for families and children—is anything but clear.
By
August 16, 2022
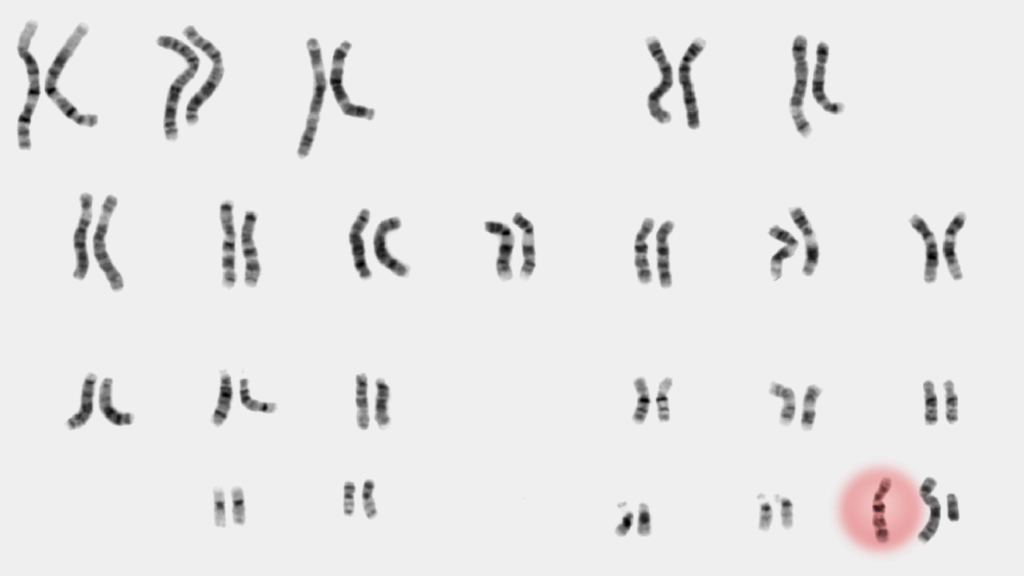
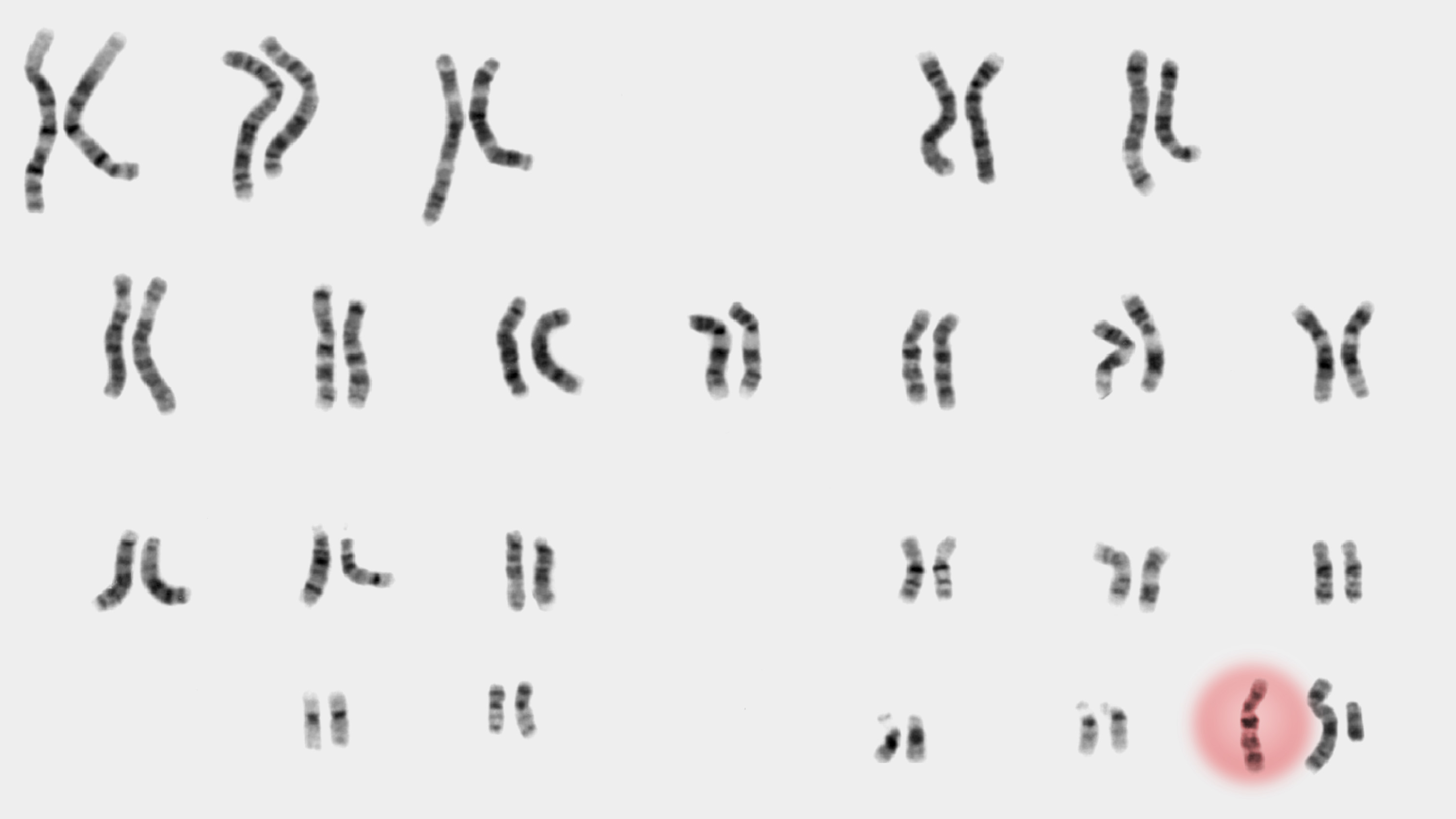 ILLUSTRATION SOURCES: NATIONAL HUMAN GENOME RESEARCH INSTITUTE
ILLUSTRATION SOURCES: NATIONAL HUMAN GENOME RESEARCH INSTITUTE
When Ollie’s mother, Katie, was nine weeks pregnant, her obstetrician-gynecologist’s office in Boulder, Colorado, offered her a special $100 price on a new prenatal blood test that she was told could detect major chromosomal hiccups such as Down syndrome and trisomy 18. She and her husband agreed—who can say no to a deal?—with one caveat. “Remember,” Ollie’s mother told the nurse, “we don’t want to know the sex.”
But they ended up finding out anyway when they received an unexpected phone call from their ob-gyn. “He said, ‘Unfortunately, I need to call and say you’re having a boy and he has XXY,’” Katie says.
Katie and her husband, Simon, had never heard of XXY, and their obstetrician wasn’t much help either. Also known as Klinefelter syndrome, XXY is a genetic condition that can cause infertility and other health issues; it occurs when a child, typically assigned male at birth, is born with an extra X chromosome in addition to the usual X and Y.
Sex chromosome variations, in which people have a surplus or missing X or Y, are the most common chromosomal conditions, occurring in as many as one in 400 births. Yet the majority of people affected don’t even know they have them. That’s because these conditions can fly under the radar; they’re not life threatening or necessarily even life limiting and don’t often have telltale characteristics that raise red flags. Still, the diagnosis can cause distress.
As more expectant parents opt for noninvasive prenatal testing in hopes of ruling out serious conditions, many of them are surprised to discover instead that their fetus has a far less severe—but far less well-known—condition. Because so many sex chromosome variations have historically gone undiagnosed, many ob-gyns are not familiar with these conditions, leaving families to navigate the unexpected news on their own. Many wind up seeking information from advocacy organizations, genetic counselors, even Instagram as they figure out their next steps.
The information landscape has shifted dramatically since the advent of noninvasive prenatal screening (NIPS) a decade ago. The increasingly popular first-trimester blood tests that debuted in 2011 to detect Down syndrome have, over time, added a broader spectrum of conditions to their panel, including sex chromosome aneuploidies—the medical name for an atypical number of chromosomes.
“The scariest part is here is this diagnosis based on a test that we didn’t really understand.”
In 2020, the American College of Obstetricians and Gynecologists endorsed NIPS at any age, effectively making the blood test a routine part of pregnancy care. Parents typically use these tests to rule out Down syndrome or more severe conditions, only to find out in many cases about something they didn’t even realize their baby was being screened for. “The scariest part is here is this diagnosis based on a test that we didn’t really understand,” says Simon. Adds Katie: “We were assuming the test would detect only very serious things.”
To add to the complexity, NIPS is not as reliable for sex chromosome aneuploidies as it is for Down syndrome, underscoring the importance of confirming a positive screening result during pregnancy via amniocentesis or chorionic villus sampling (which examines placental tissue), or with a blood sample after the baby is born. Yet data suggests that “some women have elected to terminate pregnancies solely on the basis of results, potentially aborting unaffected fetuses,” according to a 2016 article in Prenatal Diagnosis.
About 40% of men with XXY are diagnosed over the course of their lifetimes, usually when they experience fertility problems as adults, says Nicole Tartaglia, a global expert on sex chromosome variations. People with XXY may have learning difficulties and challenges with social interaction, along with physical traits such as small testes, a less muscular body, and less facial and body hair. But most people with Klinefelter syndrome grow up to live productive, healthy lives.
Meanwhile, only 10% of people with XXX or XYY are aware of their condition. But these numbers are growing as genetic testing becomes more widespread. “Judging by the number of phone calls we are getting, the proportion of those who are going undiagnosed is getting smaller,” she says.
When families learn that their fetus has a sex chromosome variation, one of the first places they turn is AXYS, the Association for X and Y Chromosome Variations, an advocacy and support organization that has seen its calls from confused families skyrocket as NIPS has become more popular. “People come to us very scared,” says Carol Meerschaert, the organization’s executive director. “They don’t know about these conditions, and their doctors don’t know about them either, but they are much more common than Down syndrome.”
XXY occurs in about one of every 650 male births; XXX affects one in 1,000 female births, and XYY one in 1,000 males. “I like to say that you have met someone with one of these conditions,” she says. “You just didn’t know it, and they may not know it!”
Related Story
Whatever happened to DNA computing?
Many alternatives to silicon have been proposed over the years. Some are finding their way into computing.
The availability of genetic counseling and information about X and Y variations isn’t keeping pace with the growing number of families learning about such variations in their unborn children. This void is what prompted Lilian Cohen, a pediatric geneticist, to help launch a center dedicated to X and Y variations at Weill Cornell Medicine in New York City. “Noninvasive prenatal testing is one of the reasons why in one week I had four patients, three of whom were diagnosed prenatally,” she says. “Couples are not getting the counseling they need.”
Depending upon what condition the screening tests are analyzing for, the accuracy of results can range significantly. “These X and Y variations are found accidentally through this technology,” says Cohen, who believes that access to genetic counseling is an essential part of testing. “My bias as a geneticist is that this knowledge is powerful.”
If people don’t go for genetic counseling after a positive screening result—few do, Cohen says—they may overestimate the severity of the condition and decide to end the pregnancy. “They may never even make it to our office,” she says. “I only see the tip of the iceberg.”
When families do come see her, she explains how different X and Y variations are from Down syndrome, which can be accompanied by heart conditions, intellectual disability, and complex congenital problems. “As much as I love my patients with Down syndrome,” Cohen says, “that is a different kind of decision-making.”
It’s a perplexing time in history to have a sex chromosome variation. We live in a world where there is confusion and mystery around the intersection of sex and gender. In fact, it’s not uncommon for people with these variations to be labeled as intersex, a term that encompasses unique variations of sex or reproductive anatomy, including genitalia, hormones, internal organs, and/or chromosomes. While some people consider sex chromosome aneuploidies like Klinefelter to be under the intersex umbrella and do identify with intersex movements, some do not. “Parents are worried that people will think their son isn’t as much of a man because they have an extra chromosome, so people don’t talk about it,” says Meerschaert. “This isn’t simple.”
Numerous companies and labs offer noninvasive prenatal screening, which analyzes tiny fragments of placental DNA that float in the gestating parent’s circulation to determine if there are chromosomal abnormalities. The global market, valued at more than $3 billion in 2021, is expected to more than double by 2028 as companies—including giants such as Illumina, Roche, and LabCorp—compete with one another to validate their tests for additional conditions.
Natera, one of the leading players, offers one of the more comprehensive screening tests. The company was fourth to market in early 2013; shortly after, a paper in Prenatal Diagnosis demonstrated its test’s ability to detect sex chromosome trisomies. Natera had previously included these trisomies as incidental findings, but after the paper’s publication, it added them as a routine part of every patient’s results. “The requisition form clearly states what is being screened for,” says Sheetal Parmar, a genetic counselor who is Natera’s vice president of medical affairs.
People with XXY may have learning difficulties and challenges with social interaction, along with physical issues, But most grow up to live productive, healthy lives.
Yet it’s a rare patient who reads all the fine print. “It’s always a challenge for people to fully understand all the things they’re being screened for,” says Parmar. “But having the information about a sex chromosome aneuploidy gives families time to prepare.”
On one hand, Katie is grateful for her son’s diagnosis “because it forces us to be aware and have a big safety net around Ollie if he ever needs it.” On the other hand, it can be a source of frustration. Is Ollie’s tendency to get teary when a task feels frustrating a consequence of XXY or just his nature? Katie wonders. (Challenges regulating emotions can characterize XXY.) “I will question how much of this should we worry about versus ‘This is who he is,’” she says. “My mama heart is always wondering, ‘Is this the thing? Do we need to freak out?’”
It can be challenging to lump all sex chromosome aneuploidies into one bucket. Symptoms can vary widely from condition to condition—girls with an extra X chromosome tend to be taller than their peers, for example, while those with just one X tend to be short—and there is plenty of variability even within the same condition.
While Ollie hasn’t needed any behavioral intervention, Robby, an eight-year-old boy with XXY who lives in Seattle, has had a different experience. His mother, Claire, also learned about her son’s extra chromosome through NIPS; she cried in a parking garage after her doctor called with the results. “I was in a prenatal yoga class where everyone was going around saying, I’m this far along and I’m having a boy or a girl,” she says. “I remember feeling jealous that things were so simple.”
 Robby was late to toilet train, and at preschool he’d knock over other kids’ toys, running around and making messes at cleanup time. On one particularly tough day, Claire asked the teacher: “Is his behavior outside the norm?” The teacher said yes.
Robby was late to toilet train, and at preschool he’d knock over other kids’ toys, running around and making messes at cleanup time. On one particularly tough day, Claire asked the teacher: “Is his behavior outside the norm?” The teacher said yes.
Robby’s prenatal diagnosis prompted Claire to seek early intervention. For starters, she called the eXtraordinarY Kids Clinic at Children’s Hospital Colorado, where she’d turned for guidance during her pregnancy. The clinic was recruiting participants for a study about emotional regulation in preschoolers with XXY, and Robby was the first child to enroll. A neuropsychiatric evaluation assigned him superior scores for language and spatial reasoning, but in terms of processing speed and adaptive skills—tasks like washing hands independently or eating with a fork—he was below average.
After being diagnosed with autism, anxiety, and ADHD, Robby has met with a battery of therapists, including an occupational therapist for managing anger and honing fine and gross motor skills. “It’s hugely affected our family,” says Claire, who has three children younger than Robby. “I didn’t think his challenges would be this significant.”
Robby’s parents have told him about his extra X by using a Lego analogy: “Everybody has a book of Lego instructions that talk about their bodies. Your Lego book has an extra page, which is why you feel things so deeply and you’re so tall.” But they do have concerns about his friends’ parents looking up the condition and pigeonholing him. “It’s his story to tell,” Claire says. “If he wants to be the Ryan Bregante of boys, that’s fine. But we want him to decide.”
Ryan Bregante, a 36-year-old photographer and internet personality, is one of the most outspoken men within the XXY community. Growing up in San Diego, he was bullied and struggled with reading, writing, and spelling, but he didn’t know much about his condition until 2017, when he attended an AXYS conference. “I met 20 guys with XXY,” he says. When he left, he spent three months surfing PubMed and scouring research papers to learn more about his genetics. He was dismayed by much of what he found: doom and gloom. “It was all ‘You’re stupid, you’re not going to amount to anything,’” he says. “When I Wikipediaed it, there was nothing but ‘rapists’ and ‘psychopaths.’” Though the stigma of those outdated stereotypes persists, Bregante works to dispel it.
In September 2017, Bregante made his first YouTube video, which was followed quickly by a website, Living with XXY, and an Instagram account where he solicits experiences from others with XXY and shares his own day-to-day. “What is positive about your life with XXY?” he asks.
“I want to show that we can live happy, successful lives,” he says. “Most men I know with XXY aren’t open about it, and neither are their families. I tell families, ‘If your son were deaf, would you act like this?’ The hardest thing about this diagnosis is we are walking around in plain sight. Keeping the diagnosis to yourself is perpetuating the shame.”
Parents of boys with XXY are used to deflecting questions about whether their sons are more feminine than boys without an extra X. That’s a driving force behind why most of the parents interviewed for this article didn’t want to be identified by their full names. It’s a conundrum: they realize that not being open about their child’s diagnosis may perpetuate stigma, but they’re not willing to risk compromising their child’s privacy.
In 2011, the year that NIPS emerged onto the scene, a review in Genetics in Medicine of published studies found that as many as 85% of parents decided to terminate a pregnancy after they received an XXY diagnosis.
It’s unclear what effect the overturning of Roe v. Wade may have on terminations of pregnancies affected by sex chromosome variations. It is plausible that the rate of abortions will decrease, but testing is not likely to become any less common. Families want to do prenatal testing in order to be better prepared for potential outcomes, and in some cases decide whether they want to terminate based on the results or pursue treatment.
Tartaglia, who runs the eXtraordinarY Kids’ Clinic, supports a somewhat unorthodox approach: giving boys with XXY testosterone shots early in infancy, when all babies undergo a “mini puberty”—a few months when hormones spike and set the stage for the development of reproductive organs.
Testosterone supplementation in baby boys with XXY is thought to support neurodevelopment. The theory is that a deficit could lead to low muscle tone or problems with speech.
Ollie’s parents say they didn’t seriously consider ending Katie’s pregnancy, but they needed to be reassured that Ollie could thrive. “Is the mountain this kid will have to climb every day so unbelievably hard that every day is a battle?” Simon asked the doctor, who said no, though he added that Ollie might grapple with learning disabilities and infertility.
To try to mitigate some of those outcomes, Ollie was enrolled in a study in which he got testosterone infusions starting at eight weeks old. In a full-day assessment at the eXtraordinarY Kids’ Clinic when he was two, he could drink from a cup, put on a jacket, thumb through a book—achievements that showed he was developing on schedule.
Five years later, at age seven, he’s continuing to meet and surpass milestones. He is in an advanced reading group at school and hasn’t needed any interventional services related to XXY. “He’s continued to thrive as a little boy,” says Katie.
In her practice, Tartaglia encounters some families that work hard to put a positive spin on their child’s diagnosis. “They say, ‘It’s okay. We can fix it,’” she says. Tartaglia gently redirects them: “Yes, we can help, but we can’t get rid of that extra chromosome.”
“Everyone has strengths and weaknesses, says Tartaglia. “We need to celebrate and embrace the idea that there is diversity in the way we all think, speak, act, and feel.”
Bonnie Rochman is author of The Gene Machine: How Genetic Technologies Are Changing the Way We Have Kids.
hide